|
Piebaldism

PIEBALDISM
*Aetiology and Clinical Appearance 
Piebaldism is inherited as autosomal dominant, congenital, stable leucoderma affecting about 1:14,000, equally distributed among men and women, and seen in all races. The most common mutations are situated in the c-kit gene (located in 4q12), encoding the transmembrane SCF/MGF tyrosine kinase receptor (Boissy & Nordlund 1997; Ezoe, Holmes et al. 1995; Fleischman, Gallardo et al. 1996; Giebel & Spritz 1991; Richards, Fukai et al. 2001) and resulting in that a subset of neural crest derived cells (melanoblasts) getting commited somewhere on their migration from the dorsal surface of the neural tube to the skin. Occasionally, individuals with piebaldism lack ganglion cells of the intestinal enteric neural plexus, which like melanoblasts, are derived from the neural crest.
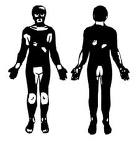
The typical piebald macules are stable, milky-white areas located in the centre of the forehead with a characteristic white forelock, ventral part of the trunk and symmetrically bilateral on the mid parts of the legs and arms. The forehead lesion of white skin and white forelock exists in about 90% of patients and is usually symmetrically central and forms an elongated triangular or diamond shape. Unlike vitiligo, the hands, feet and hips are often spared. Hyperpigmented circular macules in the border, both inside the white lesions and on the normally pigmented surrounding skin is common. These macules are darker than the normal skin and not uniformly pigmented. **See figure
Treatment
Piebaldism is often mistaken for vitiligo and for that reason patients are unfortunately put on conventional vitiligo treatment. In piebladism there are no immunological or neuropeptide background factors involved. The patients are simply born with white areas of the skin (also involving the pigmentation of the hair follicles), due to a migration fault during the early embryogenesis. Piebald skin does not respond to medical or UV-light treatments intended for generalised vitiligo. The only treatment available for Piebaldism is transplantation of melanocytes (pigment cells). On the other hand piebaldism usually responds very well to transplantation treatment with stable and long-lasting results.
We have long-term experience in transplantation of melanocytes (pigment cells) for piebaldism and have over 25 years’ successful follow-up on treated patients
*Main part of the text in this chapter is taken from the book (doctoral thesis) Vitiligo and Piebaldism by Dr Mats J Olsson, ISBN 91-554-5080-6.
**Old picture of a black girl with piebaldism, by Buffon. (From: Pearson K et al: A Monograph on Albinism in Man: Drapers' Company Research Memoirs. Biometric Series VI, Atlas, Part I. London, Dulau, 1911). The picture is truncated from the original size.
|
After more than 25 years in the field we know Piebaldism and how to fight it! |
|
|




News
Headlines »
Headlines »
New Vitiligo device:
In September 2011 The International Vitiligo Center has finalized an agreement to be a European agent for the new targeted
(focused) UBV device Levia® for the
effective treatment of vitiligo.
Headlines »
Headlines »
|